
Nociceptive vs. Neuropathic Pain: Know the Difference

Dr. Saurabh Dang
Medical Director, Hudson Pain and Spine
Nociceptive vs. Neuropathic Pain: Know the Difference
TL;DR:
- Nociceptive and neuropathic pains have different origins, requiring distinct treatments for effective relief. Recognizing the specific pain type through symptoms and patient history guides appropriate therapy and avoids futile interventions. Many patients experience overlapping pain mechanisms, demanding comprehensive, personalized management.
Nociceptive pain is defined as pain triggered by actual or threatened tissue damage, while neuropathic pain originates from damage or dysfunction within the nervous system itself. The difference between nociceptive and neuropathic pain is not just academic. It determines which treatments work, which tests matter, and how you describe your symptoms to your doctor. Approximately 20% of the population lives with chronic pain, and neuropathic mechanisms complicate diagnosis and treatment in a significant share of those cases. Getting the distinction right is the first step toward real relief.
What is the difference between nociceptive and neuropathic pain?
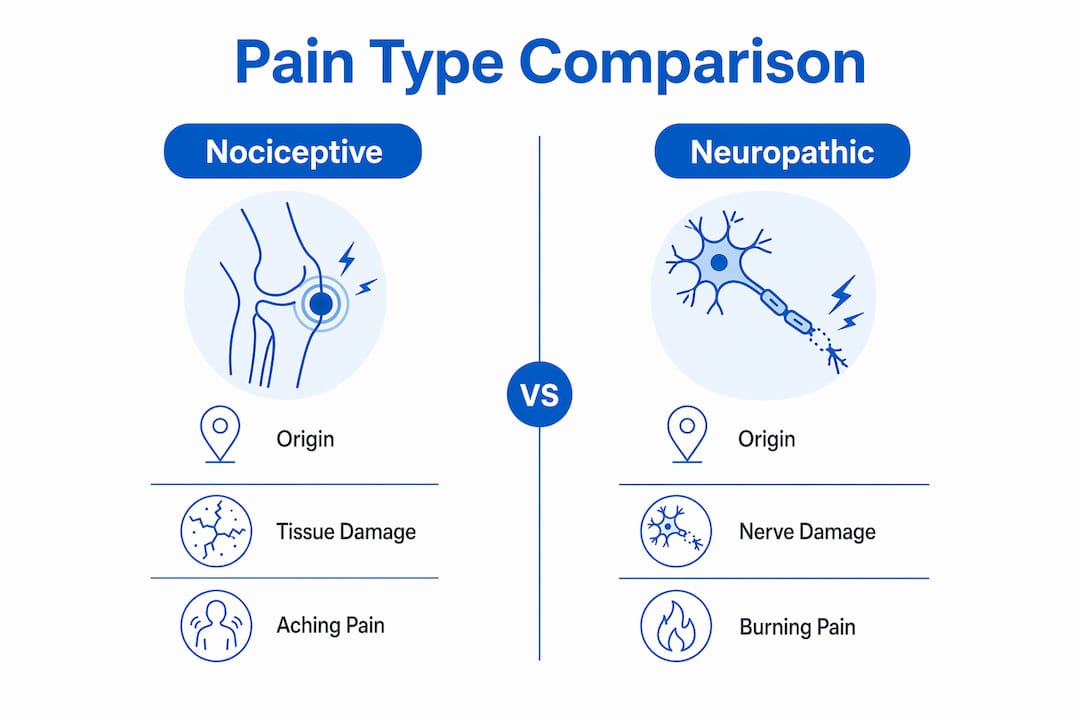
The core difference between nociceptive and neuropathic pain comes down to where the pain signal originates. Nociceptive pain starts in the body’s tissues. Neuropathic pain starts in the nerves themselves.

Nociceptive pain fires when specialized nerve endings called nociceptors detect injury, inflammation, or chemical irritation in muscles, joints, skin, or organs. The signal travels up the spinal cord to the brain, which registers it as pain. This system works exactly as intended. It tells you that something in your body needs attention.
Neuropathic pain, by contrast, arises when the somatosensory nervous system itself is damaged or diseased. The International Association for the Study of Pain (IASP) defines neuropathic pain as pain caused by a lesion or disease of the somatosensory system. The signal is not a warning about tissue injury. It is a malfunction of the wiring itself.
This distinction matters enormously for treatment. Classifying pain mechanisms is essential because nociceptive pain responds to anti-inflammatory or physical treatments, while neuropathic pain requires nerve-targeting agents or interventional therapies. Choosing the wrong approach wastes time and leaves patients in unnecessary pain.
What are nociceptive pain symptoms and how does it feel?
Nociceptive pain has a recognizable character. Most patients describe it as aching, throbbing, dull, or pressure-like. The pain tends to sit right where the injury is, making it easy to point to.
Common nociceptive pain symptoms include:
- Aching or throbbing at the site of injury or inflammation
- Dull, pressure-like discomfort, typical of muscle strains or arthritis
- Sharp pain with movement, common after fractures or surgery
- Tenderness when pressing directly on the affected area
- Gradual improvement as the underlying tissue heals
The causes of nociceptive pain are straightforward: arthritis, muscle strains, bone fractures, post-surgical tissue trauma, and inflammatory conditions. The pain is proportional to the degree of tissue damage. As healing progresses, the pain typically fades.
Nociceptive pain also responds well to treatments that address tissue inflammation. NSAIDs like ibuprofen or naproxen reduce the chemical signals that activate nociceptors. Physical therapy restores movement and reduces mechanical stress on injured tissues. Epidural injections can calm severe inflammation around spinal structures.
Pro Tip: If your pain is well-localized, worsens with movement or pressure, and started after a clear injury or flare-up, it is likely nociceptive. Tell your provider exactly where it hurts and what makes it better or worse. That specificity speeds up diagnosis.
How does neuropathic pain differ in symptoms and causes?
Neuropathic pain feels nothing like a typical injury. Patients describe it as burning, shooting, electric shock-like, or stabbing, and those descriptors are clinically meaningful. They signal nerve dysfunction rather than tissue damage.
Key neuropathic pain characteristics include:
- Burning or electric sensations that travel along a nerve pathway
- Allodynia, where light touch or clothing contact causes pain
- Hyperalgesia, an exaggerated pain response to mild stimuli
- Numbness or tingling in the affected area
- Spontaneous pain that occurs without any trigger
Common causes of neuropathic pain include diabetic peripheral neuropathy, sciatica, postherpetic neuralgia (shingles-related nerve pain), complex regional pain syndrome (CRPS), and nerve compression from herniated discs. You can read more about one of the more complex presentations in this overview of CRPS symptoms.
Neuropathic pain is also persistent. It frequently continues long after any original tissue injury has healed, because the problem lies in the nerve itself. Clinicians use validated screening tools like the DN4 (Douleur Neuropathique 4 Questions) and PainDETECT questionnaires to identify neuropathic features from patient-reported symptoms. These tools ask about the quality, location, and triggers of pain to separate nerve-driven pain from tissue-driven pain.
“Neuropathic pain is not just pain that is hard to treat. It is a fundamentally different biological process. Recognizing its hallmarks, burning, allodynia, spontaneous firing, changes everything about how we approach management.”
Pro Tip: If your pain feels like electricity, burning, or pins and needles, and it does not match a clear injury site, mention those exact words to your provider. Descriptors like ‘burning’ and ‘electric’ are red flags for neuropathic involvement and will prompt the right screening questions.
How do clinicians differentiate nociceptive and neuropathic pain?
Distinguishing between pain types in clinical practice relies more on your story than on a scan. Neuropathic pain diagnosis depends heavily on patient-reported symptoms, including timing, distribution, and quality, more than on imaging or blood work. That makes your ability to describe your pain one of the most powerful diagnostic tools available.
Clinicians follow a structured approach:
- Pain quality assessment. Providers ask whether pain is aching and localized (nociceptive) or burning, shooting, and diffuse (neuropathic). The DN4 and PainDETECT questionnaires formalize this step.
- Duration and timeline. Acute pain lasting under 3 months is often nociceptive and self-limiting. Chronic pain persisting beyond 3 months frequently involves neuropathic or nociplastic mechanisms requiring broader assessment.
- Neurological examination. Providers test for allodynia, reduced sensation, and abnormal reflexes in the painful area. These findings point toward somatosensory system involvement.
- Screening questionnaires. Tools like the DN4, PainDETECT, and S-LANSS assign scores based on symptom patterns. A high score on these tools supports a neuropathic diagnosis.
- IASP diagnostic criteria. The IASP grades neuropathic pain as possible, probable, or definite based on the combination of symptom history, clinical signs, and confirmatory tests.
One important limitation: standard imaging like MRI or CT often fails to show neuropathic pain causes because functional nerve impairment frequently lacks visible structural damage. A normal MRI does not rule out neuropathic pain. This surprises many patients who expect a scan to explain everything.
Mixed pain states add another layer of complexity. A patient with lumbar radiculopathy may have both disc-related nociceptive pain and nerve-compression-driven neuropathic pain simultaneously. Providers must weigh the full clinical picture rather than relying on a single test result.
Pro Tip: Before your appointment, write down your pain descriptors, when it started, what triggers it, and what makes it better. Bring that list. Providers who see detailed symptom notes can move faster toward an accurate diagnosis.
What are the treatment implications of knowing your pain type?
Treatment strategy changes completely depending on whether pain is nociceptive, neuropathic, or mixed. Choosing the right approach from the start avoids months of ineffective therapy.
For nociceptive pain, the first-line options target tissue inflammation and mechanical dysfunction:
- NSAIDs and acetaminophen reduce inflammation and lower pain signal intensity at the tissue level
- Physical therapy addresses the biomechanical cause and rebuilds strength around injured structures
- Corticosteroid injections deliver targeted anti-inflammatory medication directly to the pain source
- Epidural injections are effective for nociceptive spinal pain from disc herniation or spinal stenosis
For neuropathic pain, the treatment targets the nervous system directly:
- Gabapentinoids (gabapentin, pregabalin) calm overactive nerve signaling
- Tricyclic antidepressants and SNRIs (duloxetine) modulate pain processing in the central nervous system
- Topical agents like lidocaine patches reduce peripheral nerve firing at the skin level
- Nerve blocks interrupt pain signals along specific nerve pathways
- Spinal cord stimulation uses electrical impulses to override chronic neuropathic pain signals
Pain often involves multiple mechanisms, making combined therapies necessary rather than single treatments. Monotherapy frequently falls short when both tissue and nerve components are present. Patients who do not respond to a single drug class should discuss a multimodal pain treatment plan with their provider.
Pro Tip: If a treatment that worked initially stops being effective, that is a signal worth reporting. It may mean your pain has a mixed mechanism that requires a different or additional approach.
What is mixed pain and why does it complicate diagnosis?
Mixed pain is the simultaneous presence of nociceptive and neuropathic components in the same condition. It is more common than most patients realize. Lumbar radiculopathy is a classic example: the disc pressing on a nerve root creates both tissue-based nociceptive pain in the back and nerve-driven neuropathic pain radiating down the leg.
Many patients experience mixed nociceptive and neuropathic pain, which explains why monotherapy often fails. A drug that calms nerve pain may do nothing for the inflammatory component, and vice versa. Providers who miss the mixed nature of a patient’s pain often cycle through treatments without lasting success.
Tracking your symptoms carefully is one of the most practical things you can do. Note:
- Where exactly the pain is located and whether it radiates
- What it feels like (aching vs. burning vs. shooting)
- What triggers it and what relieves it
- Whether it changes throughout the day or with activity
A related concept worth knowing is nociplastic pain, a third pain mechanism recognized by the IASP. Nociplastic pain arises from altered nociception without clear evidence of tissue or nerve damage. Central sensitization, where the central nervous system becomes hypersensitive to pain signals, is the underlying driver. Conditions like fibromyalgia involve this mechanism. Understanding that three distinct pain types exist, not just two, helps explain why some patients have pain that does not fit neatly into either nociceptive or neuropathic categories.
“Mixed pain is not a diagnostic failure. It is a clinical reality. Patients with overlapping mechanisms need providers who look for both components and treat them together.”
Patients with chronic pain that has not responded to standard treatments should ask their provider directly whether a mixed or nociplastic mechanism might be involved.
Pain management at Hudson Pain and Spine
Hudson Pain and Spine provides expert evaluation and treatment for both nociceptive and neuropathic pain across Northern and Central New Jersey. Whether your pain stems from tissue inflammation, nerve dysfunction, or a combination of both, the clinical team builds individualized treatment plans that address the actual mechanism driving your symptoms.
Services range from epidural injections and nerve blocks to spinal cord stimulation and advanced interventional procedures. Hudson Pain and Spine accepts most major insurance plans and offers convenient locations across Bergen, Passaic, and Middlesex counties. If you are ready to get a clear diagnosis and a treatment plan that matches your pain type, schedule an evaluation at a convenient location.
FAQ
What is the main difference between nociceptive and neuropathic pain?
Nociceptive pain originates from tissue damage or inflammation and is detected by nociceptors, while neuropathic pain results from damage or disease within the somatosensory nervous system itself. The distinction determines which treatments are effective for each type.
Can nociceptive and neuropathic pain occur at the same time?
Yes. Mixed pain, where both nociceptive and neuropathic mechanisms are present simultaneously, is common in conditions like lumbar radiculopathy and post-surgical pain. This overlap often explains why single-drug treatments fail to provide complete relief.
How do doctors diagnose neuropathic pain without imaging?
Neuropathic pain diagnosis relies primarily on patient-reported symptom quality, timing, and distribution, supported by validated tools like the DN4 and PainDETECT questionnaires. Standard imaging frequently misses neuropathic causes because functional nerve impairment often produces no visible structural changes.
How long does pain need to last before it is considered chronic?
Pain lasting beyond 3 months is classified as chronic and often involves neuropathic or nociplastic mechanisms that require a broader, biopsychosocial assessment rather than simple tissue-focused treatment.
What treatments work best for neuropathic pain?
Neuropathic pain typically responds to nerve-targeting medications such as gabapentinoids, tricyclic antidepressants, and SNRIs like duloxetine, as well as interventional options including nerve blocks and spinal cord stimulation. The right combination depends on the specific cause and severity of the nerve dysfunction.
Recommended
- Chronic Knee Pain That Won’t Go Away? When Genicular Nerve Ablation May Help | Hudson Pain and Spine Blog
- Nerve Pain Explained: Causes, Symptoms, and Advanced Treatment Options in New Jersey | Hudson Pain and Spine Blog
- Pain Procedures Without General Anesthesia: 2026 Guide | Hudson Pain and Spine Blog
- What Is Multimodal Pain Treatment: A Clear Guide | Hudson Pain and Spine Blog
About Dr. Saurabh Dang, MD, MBA
Dr. Saurabh Dang is a double board-certified interventional pain management specialist serving Central and Northern New Jersey. He combines clinical expertise with a patient-centered approach to help patients find lasting relief from chronic pain conditions.
Read Full Bio →Seeking Treatment for Chronic Pain?
Dr. Dang and the team at Hudson Pain and Spine offer specialized care and advanced interventional treatments.
Ready to Find Relief from Pain?
Schedule your consultation with Dr. Saurabh Dang at our Englewood office.
Serving patients across Central and Northern New Jersey — Bergen, Passaic, and Middlesex counties.