
Cortisol and Chronic Pain: What You Need to Know

Dr. Saurabh Dang
Medical Director, Hudson Pain and Spine
Cortisol and Chronic Pain: What You Need to Know
TL;DR:
- Cortisol controls inflammation and influences pain sensitivity through the HPA axis. Disruption of its circadian rhythm and regulation leads to self-sustaining chronic pain. Addressing cortisol dysfunction with multimodal treatment can help break this biological lock-in and reduce pain.
Cortisol is defined as the body’s primary stress hormone, and its role in chronic pain is more central than most patients realize. Produced by the adrenal glands and regulated by the hypothalamic–pituitary–adrenal (HPA) axis, cortisol normally suppresses inflammation by blocking prostaglandins and calming immune activity. When that system breaks down under the weight of persistent pain, inflammatory cytokines go unchecked, and pain becomes self-reinforcing. Understanding this chronic pain cortisol connection is the first step toward treating pain at its biological root, not just its symptoms. Hudson Pain and Spine works with patients across New Jersey to do exactly that.
How does cortisol regulate pain and inflammation?
Cortisol’s primary job in the body is to control inflammation. When you experience an injury or acute stress, the HPA axis signals the adrenal glands to release cortisol. That cortisol then suppresses prostaglandins, the chemical messengers that drive swelling, heat, and pain at injury sites. It also dials down immune cells that would otherwise flood tissues with pro-inflammatory signals.
Cortisol also mobilizes glucose to fuel the body’s stress response. This energy shift is useful in short bursts. During a brief crisis, higher cortisol helps you respond and recover. The problem starts when that crisis never ends.
Cortisol follows a circadian rhythm. Levels peak in the early morning, around 6:00–8:00 AM, and gradually fall through the day, reaching their lowest point at night. That nighttime drop is not just rest. It is when the body resolves inflammation accumulated during the day. Chronic pain disrupts this rhythm, preventing the normal nocturnal cortisol drop and blocking the body’s nightly repair window. Patients who cannot complete that cycle wake up with inflammation that was never resolved.
Pro Tip: Track your pain levels at different times of day for two weeks. If pain consistently spikes in the morning or late evening, that pattern may reflect a disrupted cortisol rhythm worth discussing with your pain specialist.
Key ways cortisol influences pain biology:
- Prostaglandin inhibition: Cortisol blocks the enzymes that produce prostaglandins, reducing localized inflammation at injury sites.
- Immune modulation: Cortisol suppresses T-cell activity and reduces cytokine production, limiting the immune system’s inflammatory output.
- Circadian regulation: The daily cortisol cycle governs when inflammation is suppressed and when healing occurs.
- Autonomic balance: Normal cortisol patterns support parasympathetic (rest and repair) nervous system activity, which is essential for recovery.
What happens when cortisol regulation breaks down?
Chronic pain does not simply persist because of tissue damage. It persists because the body’s stress and inflammation systems get locked into a dysfunctional pattern. Pain activates the HPA axis, triggering cortisol release. But when pain never resolves, the HPA axis becomes dysregulated, producing either too much cortisol (hypercortisolism) or too little (hypocortisolism). Both states worsen pain.
Hypocortisolism is particularly common in patients with long-term chronic pain conditions like fibromyalgia. When cortisol output drops too low, the body loses its primary brake on inflammation. Inflammatory cytokines accumulate, nerves become sensitized, and pain signals amplify. Hypercortisolism, on the other hand, can suppress immune function so broadly that tissue repair stalls entirely.
“Chronic pain becomes self-sustaining through positive feedback loops in the pain-processing system. The stress level needed to sustain pain is lower than the level needed to initiate it. This means that once pain is established, it takes far less provocation to keep it going.” — Biological lock-in model of chronic pain
This concept is called biological lock-in. Once pain crosses a certain threshold, it no longer depends on the original injury. The neuroimmune system maintains it independently. That is why patients sometimes report that their pain continues long after an injury has healed on imaging.
Here is how cortisol dysfunction progresses in chronic pain patients:
- Acute pain triggers HPA activation. Cortisol rises to suppress inflammation and mobilize energy.
- Pain persists beyond normal recovery. The HPA axis stays activated, disrupting the cortisol rhythm.
- Autonomic imbalance develops. Sympathetic nervous system dominance suppresses vagal tone and reduces heart rate variability.
- Cortisol output becomes dysregulated. Either too high or too low, both states promote pro-inflammatory signaling.
- Biological lock-in occurs. Pain processing becomes self-sustaining, independent of the original stressor.
Genetics also shape how individuals respond to this cascade. Variants in the genes CYP11B1 and CYP17A1, which regulate cortisol production, explain between 4% and 18% of variability in patient-reported pain intensity. That range is significant. It means two patients with identical injuries can have very different pain experiences based on how their bodies produce and process cortisol.
What does the research say about cortisol levels and pain severity?
The evidence linking cortisol levels to pain sensitivity is growing and specific. A meta-analysis of 52 studies found that higher baseline cortisol correlates with lower pressure pain thresholds, with a correlation of r = -0.22 (95% CI -0.37 to -0.05, p = 0.01). That negative correlation means the more cortisol dysregulation present, the more sensitive a patient is to pain stimuli. It is a modest but statistically meaningful relationship across a large body of research.
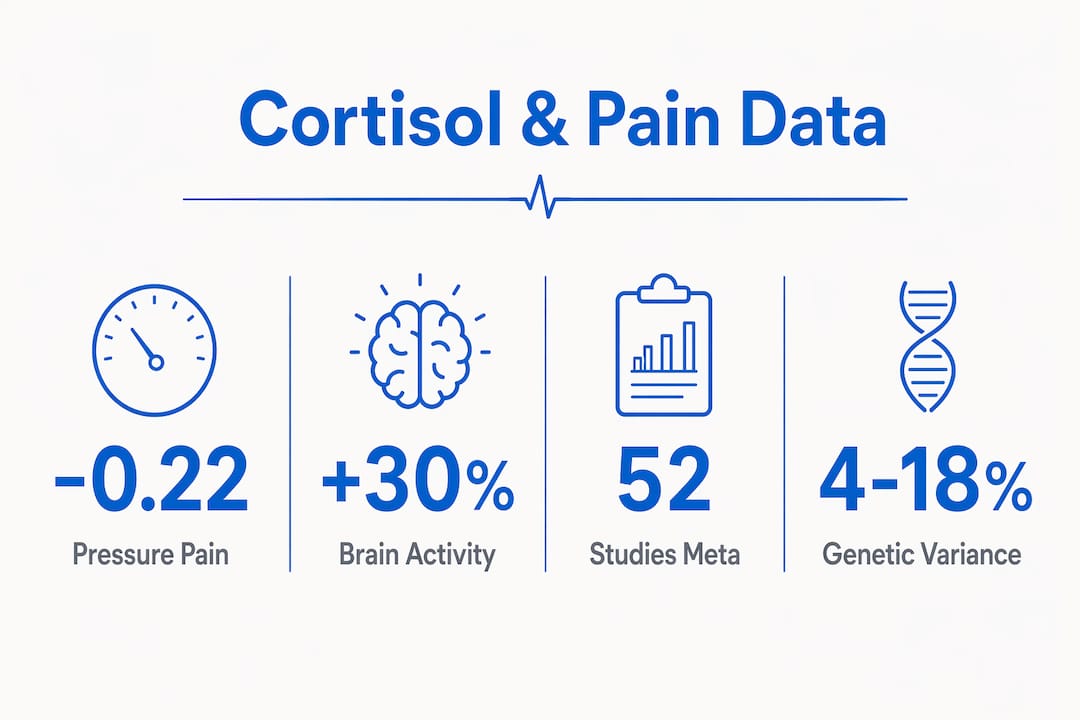
Neuroimaging adds another layer. Elevated hair cortisol levels correlate with increased resting-state brain activity in the prefrontal cortex and somatosensory regions, with correlation values of ρ = 0.45–0.47 (p < 0.01). These are the brain areas that govern cognitive and emotional processing of pain. Higher cortisol burden does not just affect the body. It rewires how the brain interprets and amplifies pain signals.
| Research finding | Key data | Clinical implication |
|---|---|---|
| Cortisol and pressure pain threshold | r = -0.22 across 52 studies | Higher cortisol dysregulation predicts greater pain sensitivity |
| CYP11B1 and CYP17A1 gene variants | Explain 4–18% of pain variability | Genetic testing may guide personalized cortisol-targeted therapy |
| Hair cortisol and brain activity | ρ = 0.45–0.47 in prefrontal and somatosensory regions | Cortisol burden alters central pain processing, not just peripheral inflammation |
| Circadian cortisol disruption | Absent nocturnal drop in chronic pain patients | Sleep-phase cortisol normalization is a treatment target |
One important caveat: cortisol is not a reliable direct diagnostic tool for measuring pain severity. Individual variability is too high for a single cortisol reading to confirm or rule out a pain diagnosis. Cortisol is better understood as a marker of overall stress-adaptive capacity. Clinicians use it as one signal within a broader clinical picture, not as a standalone test.
How can cortisol knowledge improve chronic pain management?
Knowing that cortisol dysfunction drives pain persistence changes what treatment needs to accomplish. Managing pain is not only about blocking pain signals. It requires restoring the biological systems that keep inflammation in check and allow the nervous system to reset.
Multimodal rehabilitation programs that target the biological stress response produce measurable results. A standardized five-week program involving 410 patients showed a pain intensity reduction of -0.785 points (p < 0.001), with significant improvements in affective pain metrics as well. That outcome reflects what happens when treatment addresses the full stress-pain loop, not just the symptom. You can read more about chronic pain treatment options that target these pathways.
Restoring autonomic balance is central to this approach. When the parasympathetic nervous system regains influence, cortisol rhythms can normalize, inflammation resolves more efficiently, and pain sensitivity decreases. Physical therapy plays a direct role here by improving heart rate variability and reducing sympathetic dominance through graded movement and breathing-based techniques.
Practical strategies that support cortisol regulation in chronic pain patients include:
- Sleep hygiene: Protecting the nighttime cortisol drop by maintaining consistent sleep and wake times supports the body’s inflammation-resolution window.
- Graded physical activity: Structured movement reduces sympathetic nervous system dominance and supports HPA axis normalization.
- Interventional treatments: Epidural injections and nerve blocks reduce peripheral inflammation, lowering the pain signal load that drives HPA activation in the first place.
- Stress reduction techniques: Cognitive behavioral therapy and mindfulness-based approaches reduce the psychological triggers that sustain HPA dysregulation.
- Early intervention: Treating pain aggressively before biological lock-in occurs is critical. Once the self-sustaining feedback loop is established, reversing it requires more intensive biological intervention.
Pro Tip: If you have been managing chronic pain for more than three months without meaningful improvement, ask your provider specifically about HPA axis function and circadian cortisol patterns. These are often overlooked in standard pain evaluations.
Hudson Pain and Spine’s approach to stress-driven chronic pain
Chronic pain driven by cortisol dysfunction requires more than a prescription. It requires a care team that understands the full biological picture.
Hudson Pain and Spine offers multidisciplinary pain management services across Northern and Central New Jersey. The clinical team combines interventional treatments including epidural injections, nerve blocks, and spinal cord stimulation with a patient-centered approach that accounts for hormonal and neuroimmune factors. Patients in Bergen, Passaic, and Middlesex counties can schedule care at multiple convenient locations. If you are ready to address the biological roots of your pain, not just the surface symptoms, Hudson Pain and Spine is the right starting point.
Key Takeaways
Cortisol dysregulation is a core biological driver of chronic pain persistence, not a secondary side effect, and treating it requires targeting the full HPA axis and inflammatory feedback loop.
| Point | Details |
|---|---|
| Cortisol regulates inflammation | It blocks prostaglandins and cytokines; disruption removes the body’s primary brake on pain. |
| Circadian rhythm matters | The nighttime cortisol drop resolves daily inflammation; chronic pain prevents this reset. |
| Biological lock-in is real | Once pain is self-sustaining, it requires active biological intervention to reverse. |
| Genetics influence cortisol response | CYP11B1 and CYP17A1 variants explain 4–18% of variability in pain intensity across patients. |
| Multimodal treatment works | Programs targeting the stress-pain loop reduce pain intensity with statistically significant results. |
FAQ
What is cortisol’s role in chronic pain?
Cortisol regulates inflammation through the HPA axis by suppressing prostaglandins and immune cytokines. When cortisol output becomes dysregulated under chronic pain, inflammation goes unchecked and pain sensitivity increases.
Can cortisol levels be tested to diagnose chronic pain?
Cortisol is not a reliable standalone diagnostic tool for pain severity due to high individual variability. It is more useful as a marker of overall stress-adaptive capacity within a broader clinical evaluation.
Why does chronic pain persist even after an injury heals?
Chronic pain can become biologically self-sustaining through positive feedback loops in the pain-processing system, a phenomenon called biological lock-in. Once established, this state requires less stimulation to maintain than it did to initiate.
Do genetics affect how cortisol influences pain?
Variants in the genes CYP11B1 and CYP17A1 influence cortisol production and explain between 4% and 18% of variability in patient-reported pain intensity. This means individual genetic makeup significantly shapes the cortisol-pain relationship.
What treatments help restore cortisol balance in chronic pain?
Multimodal approaches including physical therapy, interventional treatments like epidural injections, sleep normalization, and stress reduction techniques all support HPA axis regulation and help reduce pain driven by cortisol dysfunction.
Recommended
- Why Athletes Develop Chronic Pain: Causes and Solutions | Hudson Pain and Spine Blog
- Enough is enough: advanced treatment for chronic pain | Hudson Pain and Spine Blog
- Chronic Pain Treatment Options Explained for Adults | Hudson Pain and Spine Blog
- Could It Be CRPS? 4 Symptoms Beyond Chronic Pain | Hudson Pain and Spine Blog
About Dr. Saurabh Dang, MD, MBA
Dr. Saurabh Dang is a double board-certified interventional pain management specialist serving Central and Northern New Jersey. He combines clinical expertise with a patient-centered approach to help patients find lasting relief from chronic pain conditions.
Read Full Bio →Seeking Treatment for Chronic Pain?
Dr. Dang and the team at Hudson Pain and Spine offer specialized care and advanced interventional treatments.
Ready to Find Relief from Pain?
Schedule your consultation with Dr. Saurabh Dang at our Englewood office.
Serving patients across Central and Northern New Jersey — Bergen, Passaic, and Middlesex counties.