
What Is Pain Sensitization? A Guide for Chronic Pain

Dr. Saurabh Dang
Medical Director, Hudson Pain and Spine
What Is Pain Sensitization? A Guide for Chronic Pain
TL;DR:
- Pain sensitization involves abnormal nervous system responsiveness, causing pain disproportionate to tissue damage. It remains persistent due to neurobiological changes in the CNS that amplify pain signals and sustain hyper-responsiveness.
Pain sensitization is defined as a state in which the nervous system becomes abnormally responsive to stimuli, producing pain that is disproportionate to any actual tissue damage. The clinical term for this is central sensitization, a concept formally recognized by the International Association for the Study of Pain (IASP). If you live with chronic pain, you may have noticed that light touch, mild pressure, or even temperature changes trigger intense discomfort. That experience has a neurobiological explanation, and understanding it is the first step toward getting the right treatment.
What is pain sensitization and how does it affect the nervous system?
Central sensitization is a neurophysiological state in which the central nervous system (CNS) becomes hyper-responsive, producing pain from non-painful stimuli (allodynia) and exaggerated responses to painful stimuli (hyperalgesia). A meta-analysis of 54 studies with over 2,400 participants confirmed the persistence of this high-gain amplification state in CNS pain processing. That finding matters because it proves sensitization is not a psychological quirk. It is a measurable, biological change in how your nervous system operates.

The CNS essentially gets stuck in a high-alert mode. Signals that would normally be filtered out or rated as mild get amplified and broadcast as severe pain. This is why patients with fibromyalgia, for example, report widespread pain even when scans show no structural damage. The nervous system itself has become the source of the problem, not the original injury site.
Sensitization also differs from ordinary pain in one critical way. Ordinary nociceptive pain is proportional to tissue damage and resolves as healing occurs. Sensitized pain persists, spreads, and often intensifies without any new injury. Recognizing this distinction changes everything about how treatment should be approached.
How does pain sensitization work in the nervous system?
The Four-Route Central Sensitization Framework describes four key pathways that drive and sustain this condition: neuroimmune activation, glutamate-GABA dysregulation, stress-axis dysfunction, and persistent peripheral input. Each route feeds the others, creating a self-reinforcing cycle that keeps the nervous system in a pain-amplifying state.
Here is how each route contributes:
- Neuroimmune activation: Glial cells, specifically microglia and astrocytes, release inflammatory signals that increase neuronal excitability. This is not infection-based inflammation. It is a functional shift in how the brain and spinal cord process incoming signals.
- Glutamate-GABA dysregulation: Glutamate is the main excitatory neurotransmitter in the CNS. When its activity outpaces GABA, the primary inhibitory neurotransmitter, pain signals amplify rather than dampen.
- Stress-axis dysfunction: Chronic stress activates the hypothalamic-pituitary-adrenal (HPA) axis, which in turn lowers pain thresholds and disrupts normal pain modulation.
- Persistent peripheral input: Ongoing signals from an injury site, even low-level ones, can continuously feed the central sensitization cycle, keeping the CNS in a high-gain state.
Chemokine signaling pathways like CX3CL1/CX3CR1 and CCL2/CCR2 sustain chronic pain by driving glial-neuronal interactions that promote neuroinflammation and neuronal hyperexcitability. This means the immune system and nervous system are working together in a way that keeps pain alive long after the original trigger is gone.
Pro Tip: Pain sensitization involves system-wide nervous system changes, not just a localized injury response. Treating only the original injury site often fails because the real driver of pain has shifted to the CNS itself.
What are common symptoms of pain sensitization?
Symptoms of central sensitization include allodynia, hyperalgesia, widespread pain, fatigue, and cognitive dysfunction. Functional neuroimaging confirms altered activity in brain areas that process pain in patients with nociplastic pain syndromes. That imaging evidence shows the brain is genuinely working differently, not simply “overreacting.”
Allodynia means pain from stimuli that should not hurt at all, like a light brush of fabric against skin. Hyperalgesia means a stimulus that should cause mild pain causes severe pain instead. Both are hallmarks of a sensitized nervous system. Patients often describe feeling like their “pain dial” has been turned up to maximum.
Beyond pain itself, sensitization produces a cluster of associated symptoms:
- Widespread pain that moves or spreads beyond the original injury site
- Fatigue that does not improve with rest
- Cognitive changes often called “brain fog,” including difficulty concentrating and memory lapses
- Sleep disturbances that worsen pain the following day
- Heightened sensitivity to light, sound, or smell
Clinicians use the Central Sensitization Inventory (CSI), a validated self-report tool, to screen for these patterns. The CSI helps distinguish sensitization-driven pain from pain caused by ongoing tissue damage, which is a distinction that directly shapes treatment decisions.
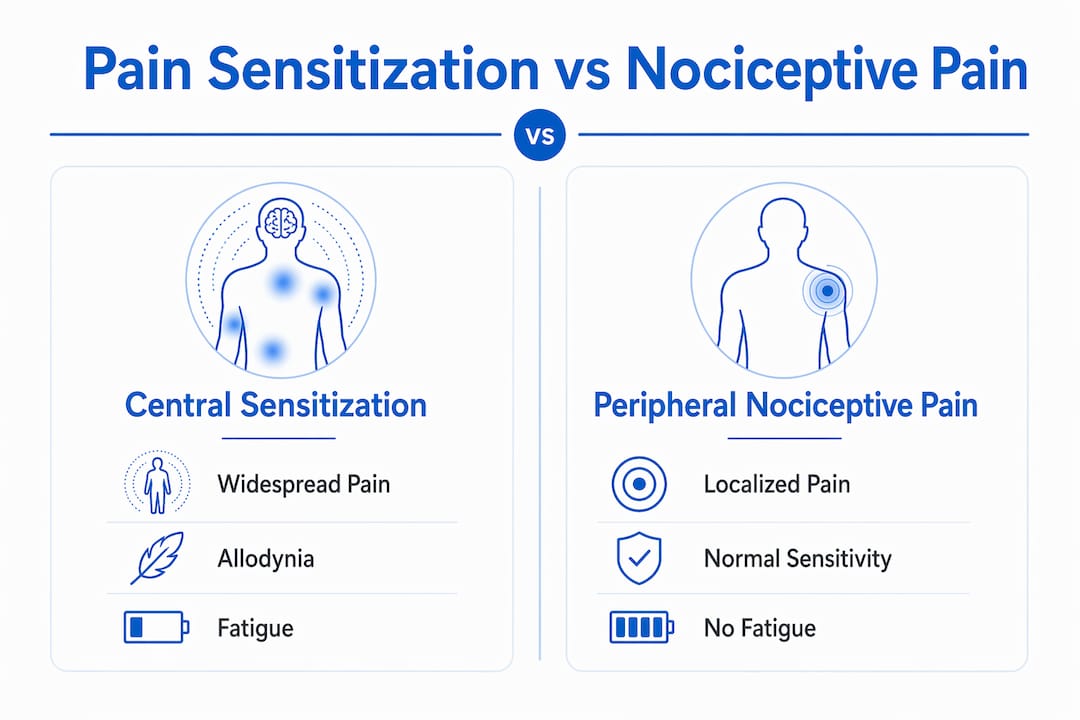
| Feature | Central sensitization | Peripheral nociceptive pain |
|---|---|---|
| Pain location | Widespread, diffuse | Localized to injury site |
| Pain trigger | Light touch, temperature, stress | Mechanical pressure, movement |
| Imaging findings | Often normal | May show structural damage |
| Response to rest | Variable, often poor | Usually improves |
| Associated symptoms | Fatigue, brain fog, sleep issues | Typically absent |
What causes pain sensitization and why does it persist?
Pain sensitization typically begins with an initial trigger: an injury, surgery, infection, or prolonged inflammation. The nervous system ramps up its sensitivity as a protective response. The problem is that, for many patients, the CNS does not return to baseline once the trigger resolves.
Central sensitization is best understood as a self-sustaining regulatory state where inhibitory capacity fails, causing the brain to amplify pain signals biologically disproportionate to actual tissue injury. Once the system tips into this high-gain state, it tends to stay there without active intervention. This is why pain can persist for months or years after an injury has fully healed.
Several factors increase the risk of sensitization becoming chronic:
- Unresolved peripheral input: Even minor ongoing signals from a healed injury site can keep the CNS primed.
- Psychological stress: Anxiety, depression, and post-traumatic stress disorder all activate the stress axis, which lowers pain thresholds.
- Sleep deprivation: Poor sleep reduces the brain’s ability to modulate pain, feeding the sensitization cycle.
- Prior pain history: Patients with a history of repeated painful episodes are more likely to develop persistent sensitization.
One common misconception is that sensitization-driven pain is “all in your head.” That framing is both inaccurate and harmful. The pain is real, measurable, and rooted in documented neurobiological changes. The brain is not imagining pain. It is generating pain through a dysfunctional but very real process.
Pro Tip: Recognizing sensitization early helps avoid unnecessary MRIs, repeat surgeries, and treatments aimed at structural problems that are not driving the pain. The right diagnosis prevents the wrong interventions.
How is pain sensitization diagnosed in clinical practice?
No single lab or imaging test diagnoses central sensitization. Diagnosis relies on clinical symptom recognition and validated tools like the Central Sensitization Inventory (CSI). Standard evaluation monitors pain intensity, emotional distress, and functional impairment over time. This approach requires a clinician who understands nociplastic pain patterns rather than one focused solely on structural findings.
Traditional MRI often appears normal in patients with pain sensitization despite severe symptoms. That normal result does not mean nothing is wrong. It means the problem is functional, not structural, and requires a different diagnostic lens.
Key elements of a clinical evaluation for sensitization include:
- Symptom pattern review: Widespread pain, allodynia, hyperalgesia, fatigue, and cognitive symptoms all point toward central sensitization.
- CSI scoring: A score above 40 on the Central Sensitization Inventory suggests clinically significant sensitization.
- Temporal summation testing: Repeated stimuli that produce escalating pain responses indicate central amplification.
- Conditioned pain modulation (CPM): Reduced CPM response signals impaired descending pain inhibition, a hallmark of sensitization.
- Functional history: How pain responds to activity, rest, stress, and sleep reveals CNS-driven patterns.
Distinguishing nociplastic pain from neuropathic or nociceptive pain is essential to avoid unnecessary surgeries and ineffective treatments. Experts stress measuring neuronal excitability changes and behavioral symptoms to inform accurate diagnosis and treatment selection. Getting this right is not just academic. It determines whether a patient gets better or cycles through treatments that cannot address the real problem.
What are effective treatment options for pain sensitization?
Treatment for pain sensitization requires a multimodal approach because no single therapy addresses all four drivers of central sensitization. Multimodal treatment targeting neuroimmune activation, autonomic dysregulation, neurotransmitter imbalance, and persistent peripheral input yields improved patient outcomes by addressing systemic nervous system dysfunction. This framework shifts the goal from “fixing the injury” to “calming the nervous system.”
Here are the primary treatment modalities, ordered by evidence strength:
- Pain reprocessing therapy (PRT): A structured psychological approach that teaches the brain to reinterpret pain signals as non-threatening. PRT directly targets the learned amplification patterns driving sensitization.
- Cognitive behavioral therapy (CBT): CBT reduces the psychological stress load that feeds the HPA axis dysfunction underlying sensitization. It is one of the most studied non-pharmacological options.
- Tricyclic antidepressants (TCAs): Level A evidence supports TCAs for reducing neuronal hyperexcitability in nociplastic pain. Dosage is titrated carefully for tolerability.
- Gabapentinoids (gabapentin, pregabalin): These medications reduce excitatory neurotransmission and are widely used for sensitization-related conditions like fibromyalgia and neuropathic pain.
- SNRIs (duloxetine, venlafaxine): SNRIs enhance descending pain inhibition by increasing serotonin and norepinephrine availability in the spinal cord.
- Physical therapy: Graded exercise and movement therapy reduce peripheral input and help recalibrate the CNS over time. Avoidance of movement worsens sensitization.
- Non-invasive brain stimulation: Techniques like transcranial magnetic stimulation (TMS) and transcranial direct current stimulation (tDCS) are emerging as adjunct options for patients with refractory sensitization.
For patients whose sensitization involves a clear peripheral driver, interventional options like nerve blocks or epidural injections can reduce the ongoing peripheral input that sustains central amplification. These are not standalone cures for sensitization, but they can reduce the signal load that keeps the CNS in high-gain mode. Reviewing chronic pain treatment options with a specialist helps identify which combination fits your specific pattern.
Hudson Pain and Spine: specialized care for pain sensitization
Chronic pain driven by sensitization needs more than a prescription. It needs a clinical team that understands the full picture.
Hudson Pain and Spine offers advanced pain management for patients across Northern and Central New Jersey. The practice provides multimodal care including nerve blocks, epidural injections, spinal cord stimulation, and Botox therapy for headaches, all tailored to address the underlying drivers of your pain. Whether your condition involves central sensitization, neuropathic pain, or a combination of both, the team builds a treatment plan around your specific pattern. Schedule a consultation at one of the convenient locations serving Bergen, Passaic, and Middlesex counties.
Key takeaways
Pain sensitization is a neurobiological condition in which the CNS amplifies pain signals beyond what tissue damage alone can explain, requiring targeted multimodal treatment rather than structural interventions.
| Point | Details |
|---|---|
| Pain sensitization definition | The CNS enters a high-gain state, producing pain disproportionate to actual tissue damage. |
| Core mechanisms | Neuroimmune activation, glutamate-GABA imbalance, stress-axis dysfunction, and peripheral input all sustain sensitization. |
| Key symptoms | Allodynia, hyperalgesia, widespread pain, fatigue, and brain fog are the primary clinical signs. |
| Diagnosis approach | No imaging test confirms sensitization; clinicians use the CSI, temporal summation, and symptom pattern review. |
| Best treatment strategy | Multimodal care combining PRT, CBT, targeted medications, and physical therapy addresses all four sensitization drivers. |
FAQ
What is the difference between central and peripheral sensitization?
Peripheral sensitization occurs at the injury site, where local nerve endings become more sensitive. Central sensitization occurs in the brain and spinal cord, amplifying pain system-wide regardless of what is happening at the original injury site.
Can pain sensitization be reversed?
Yes, with the right treatment. Pain reprocessing therapy, graded physical activity, and medications like tricyclic antidepressants and gabapentinoids can reduce CNS hyperexcitability over time. Recovery requires active nervous system down-regulation, not passive rest.
Why does my MRI look normal if I am in so much pain?
MRI detects structural damage, not functional nervous system changes. Patients with central sensitization often have normal imaging because the problem lies in how the nervous system processes signals, not in visible tissue injury.
Is pain sensitization the same as fibromyalgia?
Fibromyalgia is one condition where central sensitization is the primary driver of symptoms. Sensitization also underlies other chronic pain conditions including chronic low back pain, irritable bowel syndrome, and tension-type headaches.
How is the Central Sensitization Inventory used?
The CSI is a validated self-report questionnaire that screens for symptoms associated with central sensitization. A score above 40 indicates clinically significant sensitization and guides clinicians toward appropriate treatment strategies.
Recommended
- What Is Multimodal Pain Treatment? A Clear Guide | Hudson Pain and Spine Blog
- Chronic Pain Treatment Options Explained for Adults | Hudson Pain and Spine Blog
- Enough is enough: advanced treatment for chronic pain | Hudson Pain and Spine Blog
- Why Athletes Develop Chronic Pain: Causes and Solutions | Hudson Pain and Spine Blog
About Dr. Saurabh Dang, MD, MBA
Dr. Saurabh Dang is a double board-certified interventional pain management specialist serving Central and Northern New Jersey. He combines clinical expertise with a patient-centered approach to help patients find lasting relief from chronic pain conditions.
Read Full Bio →Seeking Treatment for Chronic Pain?
Dr. Dang and the team at Hudson Pain and Spine offer specialized care and advanced interventional treatments.
Ready to Find Relief from Pain?
Schedule your consultation with Dr. Saurabh Dang at our Englewood office.
Serving patients across Central and Northern New Jersey — Bergen, Passaic, and Middlesex counties.