
What Is Chronic Pain? Causes, Symptoms, and Relief

Dr. Saurabh Dang
Medical Director, Hudson Pain and Spine
What Is Chronic Pain? Causes, Symptoms, and Relief

Chronic pain is defined as pain that persists or recurs for longer than three months, often continuing well beyond the normal healing period for an injury or illness. Unlike a sprained ankle that resolves in weeks, chronic pain can linger without any clear ongoing tissue damage. Approximately 24% of U.S. adults reported chronic pain in 2023, making it one of the most common reasons adults seek medical care. Understanding what chronic pain is, why it develops, and how to manage it gives you a real foundation for taking the next step toward relief.
What is chronic pain and why does it last so long?
Chronic pain is not simply “a lot of pain.” It is a distinct medical condition recognized by the World Health Organization and major health authorities worldwide. The defining threshold is duration: pain lasting more than three months qualifies as chronic, regardless of whether an underlying injury is still present. That distinction matters because it shifts the focus from “what is broken” to “why is the nervous system still signaling danger.”
The brain plays a central role here. Pain is not a passive signal traveling from a wound to your brain. It is an active output your brain produces when it perceives a threat. In chronic pain, that protective alarm gets stuck in the “on” position, firing even when no real tissue damage exists. This is one of the most important and least understood facts about persistent pain.
What causes chronic pain? The role of central sensitization
Central sensitization is the leading neurological mechanism behind why pain becomes chronic. The nervous system becomes hyper-sensitive, amplifying pain signals and strengthening the pathways that carry them. Over time, stimuli that would normally feel mild, like light pressure or a slight temperature change, can trigger significant pain.
How does this happen? The transition from acute to chronic pain often follows a predictable pattern:
- An initial injury or illness triggers normal, protective pain signals.
- Inflammation and repeated signaling cause nerve pathways to become more excitable.
- The brain reinforces these pathways through neuroplasticity, essentially “learning” to produce pain even after healing.
- Pain disproportionate to the original injury emerges, along with hypersensitivity to mild stimuli, signaling that central sensitization has taken hold.
- Avoidance behaviors develop, where fear of movement reduces activity and further reinforces the pain cycle.
This process explains why two people with identical MRI findings can have completely different pain experiences. The structural picture does not tell the whole story. Stress, trauma history, and emotional states all modify how the brain processes pain, altering its intensity and limiting the effectiveness of purely physical treatments.
Pro Tip: If your pain feels out of proportion to your injury, or if light touch triggers significant discomfort, mention this specifically to your doctor. These are recognized signs of central sensitization, not exaggeration.
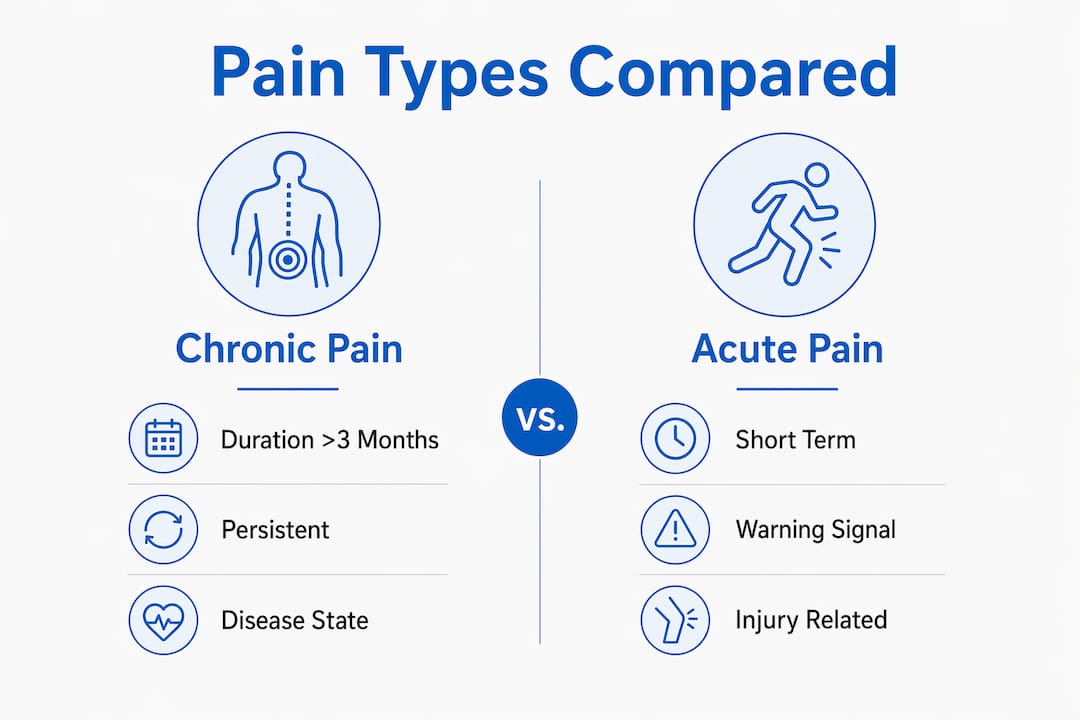
How does chronic pain differ from acute pain?
Acute pain and chronic pain serve very different purposes. Acute pain is a short-term warning signal. It tells you something is wrong and motivates you to protect the injured area while it heals. Chronic pain, by contrast, no longer serves that protective function reliably.
The WHO ICD-11 classification draws a clear line between two major categories:
| Type | Definition | Examples |
|---|---|---|
| Chronic primary pain | Pain that is itself a disease, not explained by another condition | Fibromyalgia, chronic widespread pain, complex regional pain syndrome |
| Chronic secondary pain | Pain caused by an underlying condition | Arthritis, cancer pain, post-surgical pain, diabetic neuropathy |
This distinction shapes treatment. Chronic primary pain often responds better to nervous system retraining, behavioral therapy, and neuromodulation. Chronic secondary pain requires addressing the root condition alongside pain management.
Common conditions that cause chronic secondary pain include:
- Osteoarthritis, where joint degeneration produces ongoing inflammation and pain
- Herniated discs, which compress nearby nerves and generate persistent radiating pain
- Sciatica, causing pain that travels from the lower back through the leg
- Cancer and its treatments, which can damage nerves and surrounding tissue
- Post-surgical pain, which persists in some patients even after successful procedures
Understanding which category applies to you is the first step toward choosing the right treatment path.
How does chronic pain affect mental health and quality of life?
Chronic pain and mental health are deeply connected, and the relationship runs in both directions. Pain worsens mood, and poor mood amplifies pain. Between 25% and 45% of older adults with chronic pain experience significant sleep disturbances and emotional burnout alongside their physical symptoms. That overlap is not coincidental.
The biopsychosocial model of pain explains why. This framework, now standard in pain medicine, holds that biological, psychological, and social factors all shape how pain is experienced and maintained. A patient dealing with job stress, social isolation, and a history of trauma will process pain differently than someone without those pressures, even if their physical injury is identical.
The day-to-day impact of living with chronic pain extends well beyond the physical:
- Sleep disruption reduces the body’s natural pain tolerance and recovery capacity
- Depression and anxiety are highly prevalent in chronic pain populations and worsen outcomes when untreated
- Social withdrawal develops when pain limits participation in work, family, and recreational activities
- Reduced physical activity leads to deconditioning, which can intensify pain over time
- Cognitive effects, sometimes called “pain fog,” impair concentration and memory
“Chronic pain does not just hurt. It changes how you think, how you sleep, how you relate to the people around you. Treating only the physical component while ignoring the emotional and social dimensions leaves most patients stuck.”
Pro Tip: If you notice that your pain consistently worsens during periods of stress or poor sleep, that is a clinically meaningful pattern. Share it with your care team. It points directly toward which treatments are most likely to help.
What are the most effective ways to manage chronic pain?
Managing chronic pain well requires more than one approach. The most effective strategy combines self-management with appropriate clinical care, tailored to the type and severity of pain you experience. Not all chronic pain requires aggressive medical intervention; many patients improve significantly through structured lifestyle changes and behavioral strategies.
Here is a practical framework for multimodal pain management:
- Graded movement and physical therapy. Avoiding movement because of pain reinforces fear-avoidance behavior and worsens outcomes. Structured, gradual activity retrains the nervous system and rebuilds physical capacity. Physical therapy is one of the most evidence-supported tools available.
- Cognitive behavioral therapy (CBT). CBT addresses the thought patterns and emotional responses that amplify pain. It does not mean the pain is “in your head.” It means the brain is a target for treatment, just like any other organ.
- Medications. Depending on the pain type, options include anti-inflammatories, nerve pain medications like gabapentin or duloxetine, and in some cases, carefully managed opioids. Medication works best as part of a broader plan, not as a standalone solution.
- Interventional procedures. When conservative approaches are insufficient, procedures such as epidural injections, nerve blocks, and spinal cord stimulation can provide meaningful relief. These are particularly useful for secondary chronic pain with a clear structural component.
- Neuromodulation. Spinal cord stimulation and related therapies work by altering the way pain signals travel through the nervous system. They are typically reserved for patients who have not responded to other treatments.
- Sleep and stress management. Improving sleep quality and reducing chronic stress directly reduces pain sensitivity. These are not soft recommendations. They produce measurable changes in how the nervous system processes pain signals.
Early intervention matters. The longer central sensitization goes unaddressed, the more entrenched pain pathways become. Seeking a specialist evaluation when pain crosses the three-month mark gives you the best chance of reversing the cycle before it becomes deeply established.
Key Takeaways
Chronic pain is a distinct medical condition driven by nervous system changes, not simply a symptom of ongoing injury, and effective management requires addressing biological, psychological, and social factors together.
| Point | Details |
|---|---|
| Duration defines it | Pain lasting more than three months is classified as chronic, regardless of injury status. |
| Central sensitization is the key mechanism | The nervous system becomes hyper-sensitive, amplifying pain signals beyond actual tissue damage. |
| Two major types exist | WHO ICD-11 separates chronic primary pain (pain as disease) from chronic secondary pain (pain from another condition). |
| Mental health is inseparable | Depression, anxiety, and sleep disruption both worsen and are worsened by chronic pain. |
| Multimodal treatment works best | Combining movement, behavioral therapy, and clinical interventions produces better outcomes than any single approach. |
What I’ve learned about chronic pain that most articles get wrong
After years of observing how patients and clinicians talk about chronic pain, one pattern stands out: most people still treat it as a plumbing problem. Find the leak, fix the pipe, done. That model works for a broken bone. It fails badly for chronic pain.
The patients I see who struggle most are the ones who have had every scan, every injection, every surgery, and still hurt. Not because their doctors were wrong, but because the structural focus missed the nervous system component entirely. Central sensitization does not show up on an MRI. You have to know to look for it.
What actually shifts outcomes is when patients understand that their pain is real AND that the brain is involved. Those two facts are not in conflict. Accepting both opens the door to treatments like graded exposure, CBT, and neuromodulation that would otherwise feel pointless. The biopsychosocial model is not a soft alternative to real medicine. It is the most accurate framework we have.
The other thing most articles skip: realistic expectations are not pessimism. Complete elimination of chronic pain is not always achievable. Meaningful reduction in pain and a significant return to daily function? That is achievable for most people with the right plan. That is a goal worth working toward.
Chronic pain care at Hudson Pain and Spine
Hudson Pain and Spine is a specialized pain management practice serving patients across Bergen, Passaic, and Middlesex counties in New Jersey. The practice offers a full range of interventional pain treatments including epidural injections, nerve blocks, spinal cord stimulation, and Botox therapy for headaches. Every treatment plan is built around your specific diagnosis, not a one-size-fits-all protocol. If you have been living with pain for more than three months and want a specialist evaluation, schedule a consultation at one of Hudson Pain and Spine’s convenient New Jersey locations.
FAQ
What is the medical definition of chronic pain?
Chronic pain is defined as pain that persists or recurs for more than three months. The WHO recognizes it as a distinct medical condition, separate from the underlying injury or illness that may have originally caused it.
Can chronic pain exist without an injury?
Yes. Chronic pain can persist long after an injury has healed, or develop without any identifiable structural cause. This occurs because the nervous system itself becomes sensitized and continues generating pain signals independently of tissue damage.
What is the difference between chronic primary pain and chronic secondary pain?
Chronic primary pain is pain that functions as a disease in its own right, such as fibromyalgia. Chronic secondary pain results from an underlying condition like arthritis or a herniated disc. Treatment approaches differ significantly between the two.
Does chronic pain affect mental health?
Chronic pain strongly correlates with depression, anxiety, and sleep disturbances. The relationship is bidirectional: pain worsens mental health, and poor mental health amplifies pain perception, making integrated treatment more effective than physical care alone.
When should I see a specialist for chronic pain?
Seek a specialist evaluation when pain has lasted more than three months, limits your daily activities, or has not responded to standard treatments. Early intervention reduces the risk of central sensitization becoming deeply entrenched.
Recommended
- Chronic Pain Treatment Options Explained for Adults | Hudson Pain and Spine Blog
- Why Athletes Develop Chronic Pain: Causes and Solutions | Hudson Pain and Spine Blog
- How Pain Affects Quality of Life: What You Need to Know | Hudson Pain and Spine Blog
- How your daily commute leads to chronic pain | Hudson Pain and Spine Blog
About Dr. Saurabh Dang, MD, MBA
Dr. Saurabh Dang is a double board-certified interventional pain management specialist serving Central and Northern New Jersey. He combines clinical expertise with a patient-centered approach to help patients find lasting relief from chronic pain conditions.
Read Full Bio →Seeking Treatment for Chronic Pain?
Dr. Dang and the team at Hudson Pain and Spine offer specialized care and advanced interventional treatments.
Ready to Find Relief from Pain?
Schedule your consultation with Dr. Saurabh Dang at our Englewood office.
Serving patients across Central and Northern New Jersey — Bergen, Passaic, and Middlesex counties.